This post is all about the newborn baby and the clinical examinations related with neonates.
We have discussed this topic into two parts :
A. General Appearance
Under general appearance we check for four things :
- General examinations
- Paediatrics vital signs
- Paediatrics localised examinations
- Paediatrics anthropometric measurements
I. What are the General examination we do :
- Appearance – If the baby is full-term, it should be able to move its limbs normally with a flexed posture.
- Colour of the baby – Normally appears pink but looks reddish in prematurity.
- Cyanosis – Central cyanosis which is seen on lips, tongue, mucosal membrane, conjunctiva( occurs due to cyanotic CHD, heart failure, and serious lung disease, methemoglobinemia and sulphamoglobinemia. ), Peripheral cyanosis which is seen on Hands, feet and ears( this can be seen in babies with cold stress, or the poor peripheral circulation due to hypovolaemia, shock, deep venous thrombosis, or any peripheral vascular disease ).
- Pallor – We have to examine the lips, upper surface of tongue, soles, palms, and lower bulbar conjunctiva. Skin looks pale in anaemia, shock, and generalised oedema.
- Clubbing – Create a nail with a sharper angle to the cuticle. There are mainly four grades of clubbing.
- Koilonychia – Due to iron deficiency anaemia, repeated exposure to detergent, and lichen plants, nails become soft, thin, and brittle, and the convexity of the nail is replaced by a spoon-shaped concavity.
- Capillary refill time(CRT) – This is examined by the pressing with thumb over the skin of forehead or sternum for 5 seconds, and then relaxed. Circulation normally returns in 3 seconds over the blanched area. If CTR > 3 secs , this indicates poor tissue perfusion.
- Oedema – Localised oedema( this is seen in turner’s syndrome, Milroy’s disease ), Pitting oedema( commonly seen preterm babies, heart failure, severe anaemia, and acute renal failure )
- Skin – Skin-fold thickness is checked by Harpenden’s calliper instrument. Some pathologies like Erythema toxicum, cutis marmorata, milia, salmon , mongol spot and harlequin color changes are seen.
- Jaundice – For jaundice we mainly check for Palate, Upper bulbar conjunctiva, Under surface of tongue, and Skin(Tip of nose, palms and soles)
- Jugular Venous Pressure – Because of the small neck of children under the age of two, this may not be seen.It can be viewed by forming a 45-degree angle with the bed, placing the head on a pillow, or placing a hand below the head to relax the sternocleidomastoid muscles.
II. What are the Vital signs :
Mainly there are four cardinal or vital signs and they are described below.

1. Temperature :
At the axilla, mouth, rectum, and ear, a digital thermometer is ideal. The temperature of the mouth is used as a benchmark.
- Normal temperature : 36.5°C – 37.5°C
- Cold stress : 36.0°C – 36.5°C
- Hypothermia : <36.5°C
- Hyperthermia : >37.8°C
2. Pulse/Heart Rate :
When the baby is peaceful or asleep, count the pulse by palpating the femoral pulse or the heart rate by auscultating over the precordium.
We determine the Rate,Rhythm,Volume,Character, Radio-femoral delay, Radio-radial delay, arterial wall condition.
- Normal heart rate : 120-160/min
- Heart rate during asleep : 70-80/min
- Tachycardia : >160/min
3. Blood Pressure:
This can be measured by two methods, Flush method and Auscultatory-Palpatory method. Sometimes doppler method is most correct if available.
4. Respiration :
This should be examined when the baby is quiet or sleeping.
- Normal rate : 40-60/min
- Tachypnoea : >60/min
- Periodic breathing : normal, specially in preterm babies
III. What are the Localised examination of paediatrics :
- Head Region
- Hair structure
- Face
- Teeth
- Tongue
- Tonsils
- Eyes
- Nose
- Ear
- Neck
- Paranasal air sinuses
- Body/Trunk
- Limbs
- Genitalia
1. Head Region :
During head examination, we mainly check for :
- Shape : Because of the malleable head, there is a wide variety of head size and shape, which is greatest during the infancy period. After vaginal delivery, prominent occiput, overlaying of skull bones, caput, or cephalohematoma are prevalent. Flattening of one side of the head in a child should be carefully inspected to rule out tightening of the sternomastoid muscle; otherwise, preference head posture in one side while resting supine is usual.
- Head circumference : Non-stretchable tape is placed anteriorly over the nasion and supraorbital ridges, and posteriorly across external occipital protruberance to determine it. (Normal head circumference = 33-35 cm)
- Is the skull of soft or thin/Craniobates : The skull’s capacity to indent under pressure and return to its original shape, similar like a ping-pong ball.This is a common occurrence in babies, particularly around the lambdoid sutures. Consider poor bone mineralization, as observed in rickets, if symptoms linger beyond the first six months.
- Moulding : When a baby is born head-first, pressure in the birth canal might cause the head to form into an oblong shape. The baby’s head can change shape thanks to the gaps between the bones. The overlaying of cranial bones at suture lines is most noticeable in the vertex presentation. Moulding vanishes after 7 days.
- Fontanels : In a new born there should be presence of six fontanels : (i) Anterior and posterior fontanels each 1 in number, (ii) antero and postero lateral each 2 in number.
- Brachycephaly : Brachycephaly is a condition that causes the rear of the skull to flatten out.
- Cephalhaematoma : A cephalohematoma is a blood clot that forms beneath the scalp. Small blood veins on the fetus’s head are broken as a result of slight trauma during the birth process.
- Caput succedaneum : A newborn’s caput succedaneum is a swelling of the scalp. During a head-first (vertex) delivery, pressure from the uterus or vaginal wall is the most common cause.
- Craniosynostosis : Craniosynostosis is a congenital condition in which the bones of a baby’s head fuse together prematurely. This occurs before the baby’s brain has completed its development. The skull might become increasingly deformed as the baby’s brain develops.
- Sub-aponeurotic bleeding : Bleeding behind the galea aponeurosis, which covers the scalp, is known as subaponeurotic or subgaleal haemorrhage. Because the galea aponeurotica layer is continuous throughout the scalp, bleeding in this layer is possible.
2. Hair structures :
Hair changes could be the first indicator of a serious systemic or hereditary problem.
- Ectodermal dysplasia : This is characterised by extremely thin and scant hair.
- Hyperthyroidism : Hair loss is prevalent in this case.
- Hypothyroidism : coarse hair is seen in this scenario.
- Protein-energy deficiency : changes in colour and texture of hair is seen.
3. Mouth cavity :
Examine the colour of the lips in relation to the family’s genetic ancestry. It is possible to discern cleft lips or palates. Using a tongue depressor, gently press across the base of the tongue to inspect the mouth and subsequently the throat.
- Herpes simplex virus infection : Cold sores from a herpes simplex infection can be seen.
- Candida infection : as well as crackling on the side of the mouth from a .
- Smell breath for an irritating odour of a throat or sinus infection.
- Also the acetone odour of ketosis, which is seen in famine and insufficient calorie intake, or DKA.
4. Teeth :
Look for any abnormalities in shape or dental caries; with
- Ectodermal dysplasia
- Peg-shaped teeth are common.
- The timing of the first tooth eruption is widely diverse, although a significant delay can suggest hypothyroidism or a general skeletal maturation delay.
5. Tongue :
- Hypothyroidism, Beck-Weideman syndrome, and mucopolysaccharidoses are all associated with a large protruding tongue.
- Streptococcal infection is characterised by enlarged red papillae, also known as “strawberry tongue.”
- The tongue of a healthy person is wet and sparkling, whereas a dehydrated person’s tongue is dry and hard.
- A lack of papillae on the tongue is linked to a vitamin B12 deficiency.
6. Tonsils :
Tonsils are lymphoid glands that lie between the anterior and posterior pillars and range in size from unnoticeable in newborns to achieving maximum size between the ages of 6 and 9, after which they begin to involute. Examine their size, colour, and exudate presence. Even kissing tonsils doesn’t make swallowing or breathing difficult.
7. Eyes :
- Hypertelorism : Hypertelorism, or orbital hypertelorism, is an unusually high distance between two organs or body parts. It usually refers to an increased distance between the orbits (eyes). The distance between the inner eye corners and the distance between the pupils is higher than normal in this disease.
- Eye slants :The upper and lower eyelids, which make up the form of the eye, are known as palpebral. The slant of the eye, or palpebral slant, is determined by a line drawn from the inner corner to the outer corner. Upward slant that is Mongoloid is seen in Down syndrome, and Downward that is antimongoloid is seen in Treacher Collin syndrome.
- Pupillary reflex : This starts to present after 28-30 weeks of gestational age. Leukocoria or white pupillary reflex is seen in – Chorioretinitis, Congenital cataract, Retinopathy prematurity, and persistent hyper plastic primary vitreous.
- Iris : Aniridia is a rare form of congenital absence., other common abnormalities are Coloboma, and Brush field spots in Down syndrome.
- Cornea : Normal size of cornea is 10 mm diameter, and if it is >10mm then this suggests congenital glaucoma in in term mature babies.
- Subconjunctival haemorrhage : Sub-conjunctival haemorrhage is a common condition that is typically insignificant but can occasionally signal a major medical problem. It happens when a small quantity of bleeding occurs beneath the conjunctiva, and it looks like a bruise. This incident is very common after vaginal delivery and forceps delivery then it starts to absorb gradually.
- Superficial retinal haemorrhage : Large superficial retinal veins rupturing into the space between the retina and the vitreous; these bleeding may burst into the vitreous cavity. This is observed in many newborns, usually gets absorbed gradually.
- Coloboma of eyelid : This is an eyelid deficiency due to a congenital defect. Eyelid coloboma shows as a notch in the lid’s edge, most usually in the upper lid.
8. Nose :
- A foreign body or blocking polyp could be causing offensive discharge from one of the openings.
- Active nares – Active nares should not be overlooked; they may suggest underlying pneumonia or heart failure discomfort.
- Allergic salute – In children with allergies, a “allergic salute” is a horizontal furrow across the lower half of the nose.
- Choanal atresia – This can be unilateral or bilateral.
- Congenital Syphilis – Sero-sanguinous discharge through the nose can be seen.
9. Ear :
The examiner looks for :
- Low set ear : If you extend a horizontal line from the medial canthus laterally to cover the ear, more than 10% of the ear is generally above this line.
- Congenital malformation of ear
- Preauricular skin tag
10. Neck :
- Sternomastoid tumour : A sternocleidomastoid tumour of childhood, also known as fibromatosis colli of childhood, is an uncommon benign tumour in the side of the neck muscle. The tumour is frequently on the right side and is firm with a diameter of a few centimetres. It normally appears between the second and fourth weeks of life in a newborn.
- Excessive skin folds : Also called webbing and this is seen in Turner Syndrome.
- Other rare cases : There are some rarely occurring cases like Cystic hygroma, Branchial cyst and Congenital goitre.
- And all the Cervical group of lymph nodes should be checked carefully.
Cervical LNs:
Transverse group: submental, submandibular, preauricular, postauricular and occipital.
Vertical group : Jugulo-digastric and Omohyoid group of lymph nodes.
Midline group: Prelaryngeal and pretracheal.
Superficial and deep groups related to the sternomastoid
11. Paranasal air sinuses :
Sinuses are infection hotspots that go unnoticed. The ethmoidal and maxillary sinuses are present from birth, whereas the frontal sinuses develop between the ages of 4 and 7. To evoke sinusitis sensitivity, gently press.
12. Body/Trunk :
- Trunk-limb ratio : The umbilicus is usually the halfway of length. and in abnormal case short limbed dwarfism is seen in Achondroplasia.
- Abdominal wall defect : Midline defect is seen in Omphalocele and Lateral defect is seen in Gastroschisis.
- Spine : There are mainly two problems of spine that is Kyphoscoliosis, Tuft of hair, and lipomatous swelling over spine which indicates underlying spina bifida.
- Pilonidal sinus : This is a common skin dimple which overlies the coccyx at the midline gluteal cleft. This is a common dermal sinus which is benign and asymptomatic.
- Diastasis recti which is a common finding in newborn
- Umbilical sepsis or discharge
13. Limbs :
- Hemihypertrophy : Hemihypertrophy, also known as hemihyperplasia, is a disorder in which one side of the body, or a portion of it, is larger than the other. Beckwith-Wiedemann syndrome and Russell-Silver syndrome are two congenital syndromes linked to hemihypertrophy.
- Oedema feet : Oedematous feet which is seen in Turner syndrome, and congenital lymphedema.
- Nerve plexus injury : Mainly the brachial plexus injury is involved.
- Club foot deformity
- Congenital dislocation of hip
- Arthrogryposis
- Amniotic constriction band
- Syndactyly and polydactyly
14. Genitalia :
- Uretral opening site : Normal, hypospadias and episapadius.
- Ambiguous genitalia
- Transitory hydrocele
IV. What are the Anthropometric measurements :

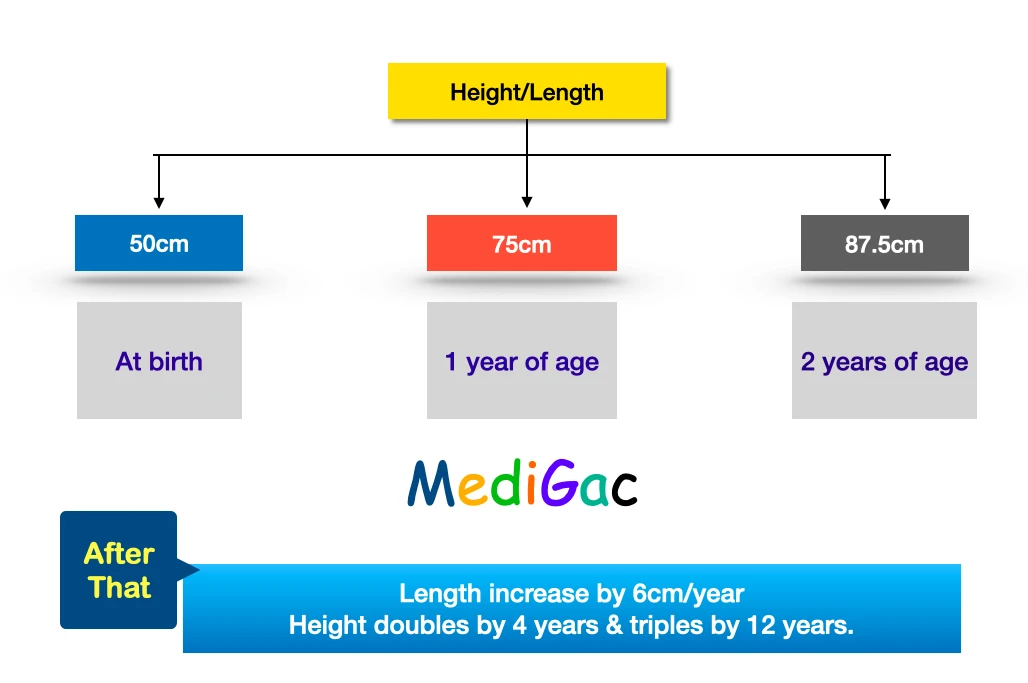
1. Height/Length :
- Length – This measured for childrens upto 2 years of age. The device which is used to take length is Stadiometer.
- Height – This is measured in childrens who are greater than 2 years of age. The device which is used to measure height is Infantometer.
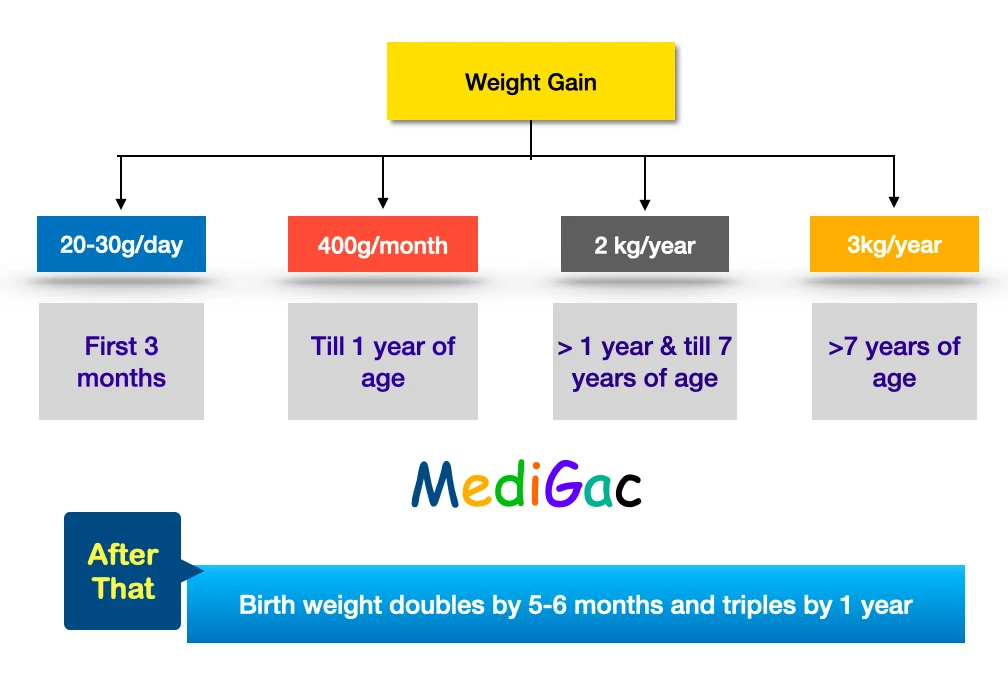
2. Weight :
Instruments to measure the weight are – weighing machine or scale : digital weighing scale, spring balance(Pan type and Platform types) and Lever type of balance.
3. Body mass index(BMI) :
This is calculated by taking weight in kg and height in meter2 .

Incase of newborns the result of BMI is interpreted by percentile :
| Girls | Boys |
| 1. Birth – 2 years : Click Here 2. 2 years – 5 years : Click Here 3. Birth – 5 years : Click Here | 1. Birth – 2 years : Click Here 2. 2 years – 5 years : Click Here 3. Birth – 5 years : Click Here |
- ≥95th percentile – Obesity
- ≥94th-85th percentile – Overweight
- 84th-5th percentile – Normal
- <5th percentile – Underweight
4. Head circumference :
The circumference of a child’s head around its biggest area is measured. It gauges the distance between the brows and ears, as well as around the back of the head.
Non-stretchable tape is placed anteriorly across the supraorbital ridges and glabella, and posteriorly over the external occipital protruberance to measure it.
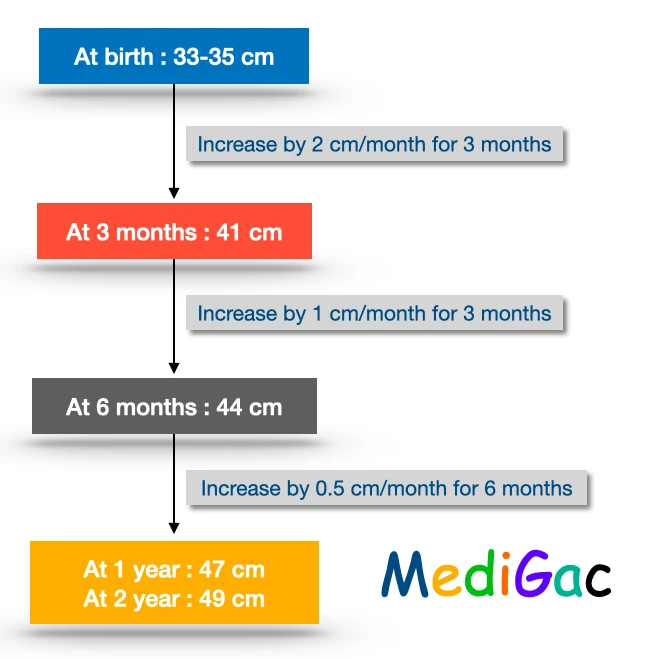
Normal values :
- At birth : 33-35 cm
- At 3 months : 41 cm
- At 6 months : 44 cm
- At 1 year : 47 cm
- At 2 years : 49 cm
Then around 5-6 years of age, adult head circumference is achieved.
5. Mid-arm circumference :
- This is taken between two points that is olecranon at the back of elbow and the acromion process at the shoulder.
- The measurement is made by a non-stretchable tape around the arm at the midpoint. Normally we use Shakir’s tape.
- Between 1-5 years of age – the normal value is 15-17cm.
- If the measurement is <15 cm : This suggests Malnutrition.
- If measurement is <11.5cm : This suggests Severe Malnutrition.
6. Chest circumference :
- This indicates nutritional status of the child.
- This is measured by a non-stretchable tape.
- And measured at the level of nipple or xiphisternum in mid-inspiration condition.
- At birth Head circumference> chest circumference ; 3 cm
- At 1 year : HC=CC
- >1 year : HC<CC
Pathology :
If At birth HC>>>CC ; then probable causes may be :
- IUGR
- Preterm baby
- Hydrocephalus
7. Upper segment and Lower segment ratio :
- Upper Segment – This is the measurement of length between upper border of symphysis pubis and the heel.
- Lower Segment – This is the measurement of length between vertex and upper border of symphysis pubis.
US:LS ratio :
- At birth – 1.7 : 1.0
- At 1 year – 1.5 : 1.0
- At 10 years – 1.0 : 1.0
- At 18 years – 0.9 : 1.0
8. Arm Span :
It’s the distance between the tips of two upper limbs’ middle fingers when they’re stretched out at a right angle to the trunk.
- Arm span < height by 1-2cm : upto 5 years of age
- Arm span = height : at 10-12 years of age
- Arm span > height by 1-3 cm : above 12 years of age
B. System wise examination
We have discussed total of seven systems. And they are discussed below.
- Cardiovascular system
- Respiratory system
- Gastro-Intestinal system
- Musculo-Skeletal system
- Genital and Urinary system
- Nervous system
- Paediatrics dermatology or skin disaeases
1. Paediatrics cardiovascular system examination :
In cardiovascular system examinations we check for :
- Common congenital disorders
- Common presenting complaints
- Inspection
- Palpation
- Auscultations
Get the full examination in details in the given below button.
2.Paediatrics respiratory system examination :
During the respiratory system examination we check for this.
- Common congenital disorders
- Common presenting complaints
- Inspection
- Palpation
- Percussion
- Auscultations
Get the full examination in details in the given below button.
3. Paediatrics gastrointestinal system :
During the the Gastro-intestinal/Alimentary system examination we check for this.
- Common congenital disorders
- Common presenting complaints
- Inspection
- Palpation
- Percussion
- Auscultations
Get the full examination in details in the given below button.
4. Musculo skeletal system :
During the Musculo-skeletal system examination we check for this.
- Common congenital disorders
- Common presenting complaints
- Inspection
- Palpation
- Percussion
Get the full examination in details in the given below button.
5. Genital and urinary system :
During the Genito-Urinary system examination we check for this.
- Common congenital disorders
- Common presenting complaints
- Inspection
- Palpation
- Percussion
- Auscultations
Get the full examination in details in the given below button.
6. Nervous system :
During the Nervous system examination we check for this.
- Common congenital disorders
- Common presenting complaints
- Tendon reflex
- Newborn reflexes
- Cranial nerve examinations
Get the full examination in details in the given below button.
7. Paediatric Dermatology(Skin diseases) :
During the respiratory system examination we check for this.
- Common congenital disorders
- Common presenting complaints
- Inspection
Get the full examination in details in the given below button.