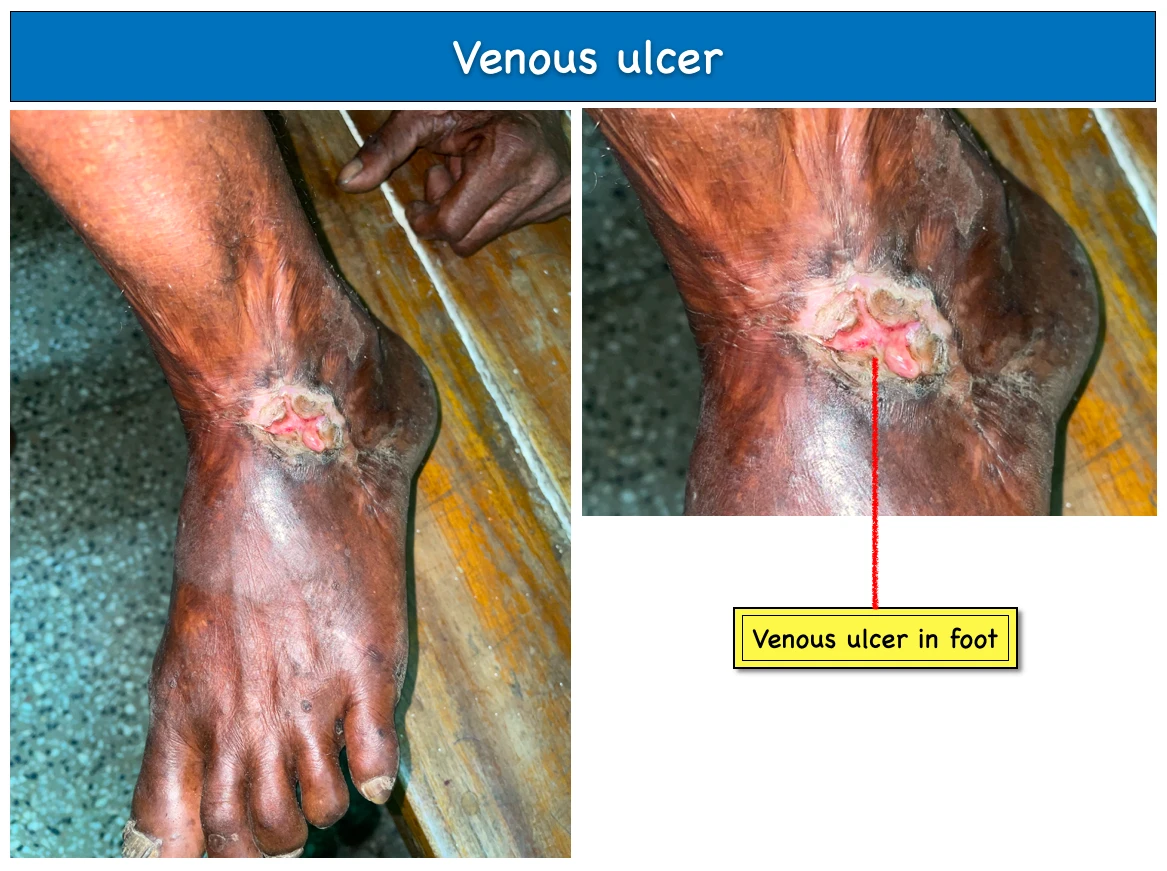
These are open sores on the ankle or lower leg are referred to as venous ulcers, sometimes known as venous stasis ulcers or non-healing wounds. They take weeks, months, and occasionally even longer to recover.
1. Clinical features :
- A venous ulcer typically has a gently sloping edge, granulation tissue on the floor, and varying amounts of slough and exudate on top of it.
- Advanced venous ulcer forms thickened, pigmented and inflamed skin.
2. Pathophysiology :

- At first due to some pathology inside the body, venous pressure gets increased. Then it causes Dilatation of vein and capillaries, Capillary perfusion pressure decreased, Endothelial tissue decrease and Capillary permeability increase.
- Then WBC trapping and Pericapillary fibrin deposition occurs. This leads to two results, one is Decreased lymphatic drainage and another one is collection of results( Not efficient tissue perforation, Reactive oxygen species develops and generates free radicals, Proteolytic enzymes increased, Growth factors inhibited) and which leads to Formation of ulcer and delayed or poor wound healing.
3. Investigations :
- Duplex Scan : To assess the status of the deep and superficial veins.
- Blood for : CBC, Glucose, ESR, CRP.
- Biopsies : This is indicated if any malignancies are suspected.
4. Treatment :
- Compression technique : By using Orthopaedic wool, Cotton crepe, Elastic bandage, Cohesive bandage.
- Superficial veinous surgery : Reducing venous hypertension to treat superficial reflux.
- Pentoxifylline : Decreased plasma cellular viscosity and cytokine inhibition result in an increase in microvascular perfusion.
- Biological dressing : Keratinocytes and collagen meshes, this has shown improvement of healing.
- Pinch graft and ulcer excision with mesh grafting.