We have discussed all the four heart sound with normal and abnormal characteristics.
A. First heart Sound (S1) :
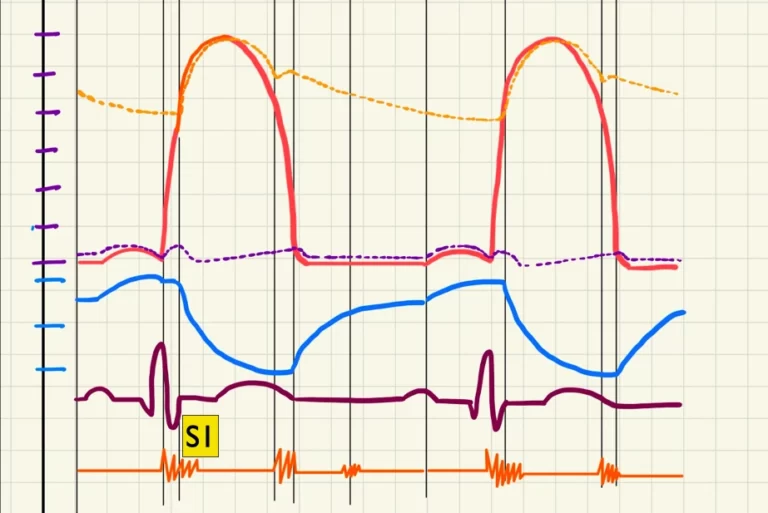
I. Description :
The First Heartbeat (S1) The shutting of the mitral and tricuspid valves causes the first heart sound. The sound produced by the mitral valve closing is known as M1, while the sound produced by the tricuspid valve closing is known as T1.
This sound is beast heard at the level of apex of the heart.
II. Pathology/Abnormality :
- If the sound is QUIET – Then it helps to diagnose various conditions like ; Low cardiac output, Long P-R interval or first degree heart block, Rheumatic mitral regurgitation and poor left ventricular function.
- If the sound is LOUD – The this loud noise can be sign of Mitral stenosis, Short P-R interval, Increased cardiac output and large stroke volume also.
- If the sound is VARIABLE – This condition mainly the sign of Complete heart block, Atrial fibrillation, and Extrasystoles.
Splitting of S1 :
Because T1 is substantially weaker than M1, a split S1 heart sound is best detected at the tricuspid listening post(Left 5th Intercostal space, along the sternal border).
The M1 sound occurs just before the T1 sound. Only a single cardiac sound is usually heard because the mitral and tricuspid valves collapse virtually simultaneously.
Although a “split S1” sound can be heard in 40 percent to 70 percent of healthy people, as well as in certain cardiac disorders. When the mitral valve closes significantly before the tricuspid valve, each valve produces a distinct audible sound.
Occurs in :
- RBBB
- Ventricular tachycardia
B. Second heart Sound (S2) :

I. Description :
At the end of systole, the aortic (A2) and pulmonary (P2) valves close, producing the second heart sound (S2). Take a listen to the audio example provided below.
P2 is better heard in the pulmonary area(Left parasternal area and at the level of 2nd intercostal space), while A2 is best heard in the Aortic area(Second right intercostal space).
II. Pathology/Abnormality :
- If the sound is QUIET – Then it is the diagnosis of Low cardiac output, Aortic regurgitation, and Calcific aortic stenosis.
- If the sound is LOUD – It indicates Systemic hypertension and Pulmonary hypertension.
- If the sound is SPLITTING – this kind of noise indicates Right and Left bundle branch block, pulmonary hypertension, Atrial and Ventricular septal defect, Aortic and Pulmonary stenosis and Hypertrophic Cardiomyopathy.
Splitting of S2 :
Because P2 is substantially weaker than A2, a split S2 is best heard at the pulmonic valve listening post(Left sided 3rd Rib or Left 3rd intercostal space across the sternal border.).
In roughly 90% of persons, S2 is biologically divided. Persistent (widened) splitting, fixed splitting, paradoxical (reversed) splitting, or no splitting can be heard in the S2 heart sound.
- Physiological Split S2 : During inspiration, greater venous return to the right side of the heart delays pulmonic valve closure (major effect), whereas decreased return to the left side of the heart speeds up aortic valve closing (small effect), further separating A2 and P2.
2. Paradoxical Split S2 : Any condition that delays the closure of the aortic valve, such as severe aortic stenosis, hypertrophic obstructive cardiomyopathy (HOCM), or a left bundle branch block, results in a paradoxical split S2 (LBBB).
3. Narrow Split S2 : When the pulmonary valve shuts early (e.g., pulmonary hypertension) or the aortic valve closes late (e.g., Aortic Stenosis), the S2 is narrowly split. This is a rare occurrence in a healthy child.
4. Widened/Persistent Split S2 : When both A2 and P2 are audible throughout the respiratory cycle, the splitting becomes more pronounced during inspiration (due to increased venous return) and less pronounced during expiration.
C. Third heart Sound (S3) :

I. Description :
It is mostly physiological or normal at young adults, pregnant females, children, but sometimes it is also pathological when the patients is more than 40 years of age.
It’s best heard at the right or left lower sternal border, in the epigastrium, or on rare occasions across the jugular veins.
II. Pathology/Abnormality :
The common causes behind this pathology are – Left ventricular failure, Mitral Regurgitation and in heart failure(here it occurs with a tachycardia which is known as “gallop” rhythm)
D. Fourth heart Sound (S4) :
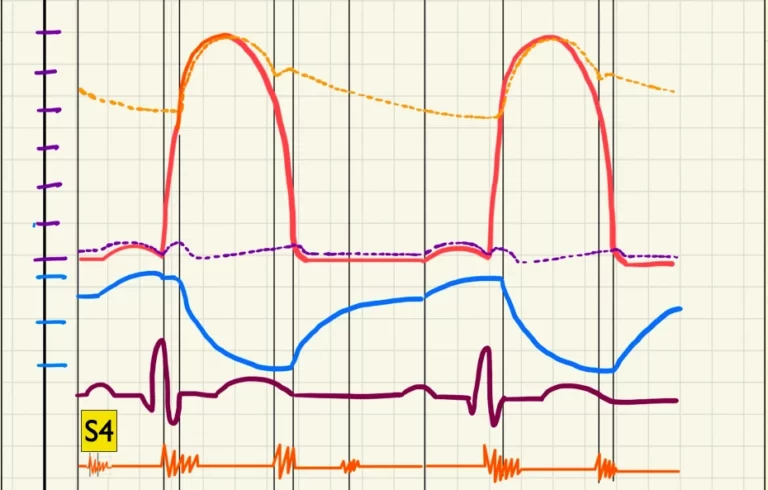
I. Description :
When the atria contract to pump blood into the left ventricle, the fourth heart sound (S4), commonly known as the “atrial gallop,” occurs right before S1. The blood striking the left ventricle produces an S4 if the left ventricle is noncompliant and atrial contraction drives blood through the atrioventricular valves.
The bell of the stethoscope should be placed near the lower left sternal border or subxiphoid area to hear a fourth heart sound coming from the right ventricle.
II. Pathology/Abnormality :
This sound is always pathological. The reasons behind this sound are left ventricular hypertrophy and forceful atrial contraction against a stiff or non-elastic ventricle.