We have discussed five topics of cardiac murmurs and they are :
- Definition of cardiac/heart murmurs
- Mechanisms of cardiac/heart murmurs
- Grades of cardiac/heart murmurs
- Types of cardiac/heart murmurs
- Loudness of cardiac/heart murmurs
I. Definition of cardiac murmurs :
This is the sound produced from flowing of blood inside an abnormal or defective heart. Abnormality may be due to valve, Hypertrophic cardiac myopathy, Ventricular septal defect etc.
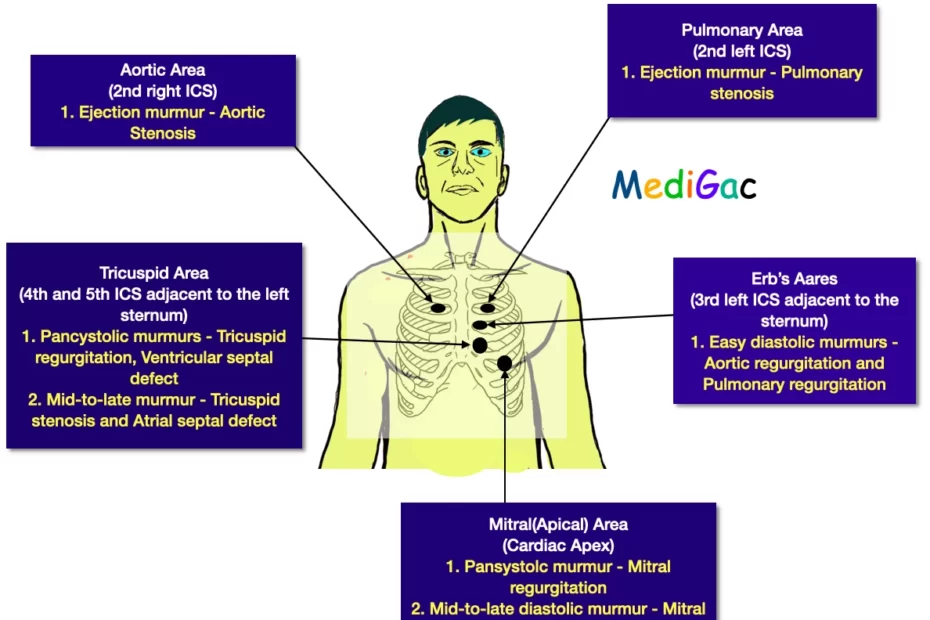
Area of chest where we get various types of murmurs :
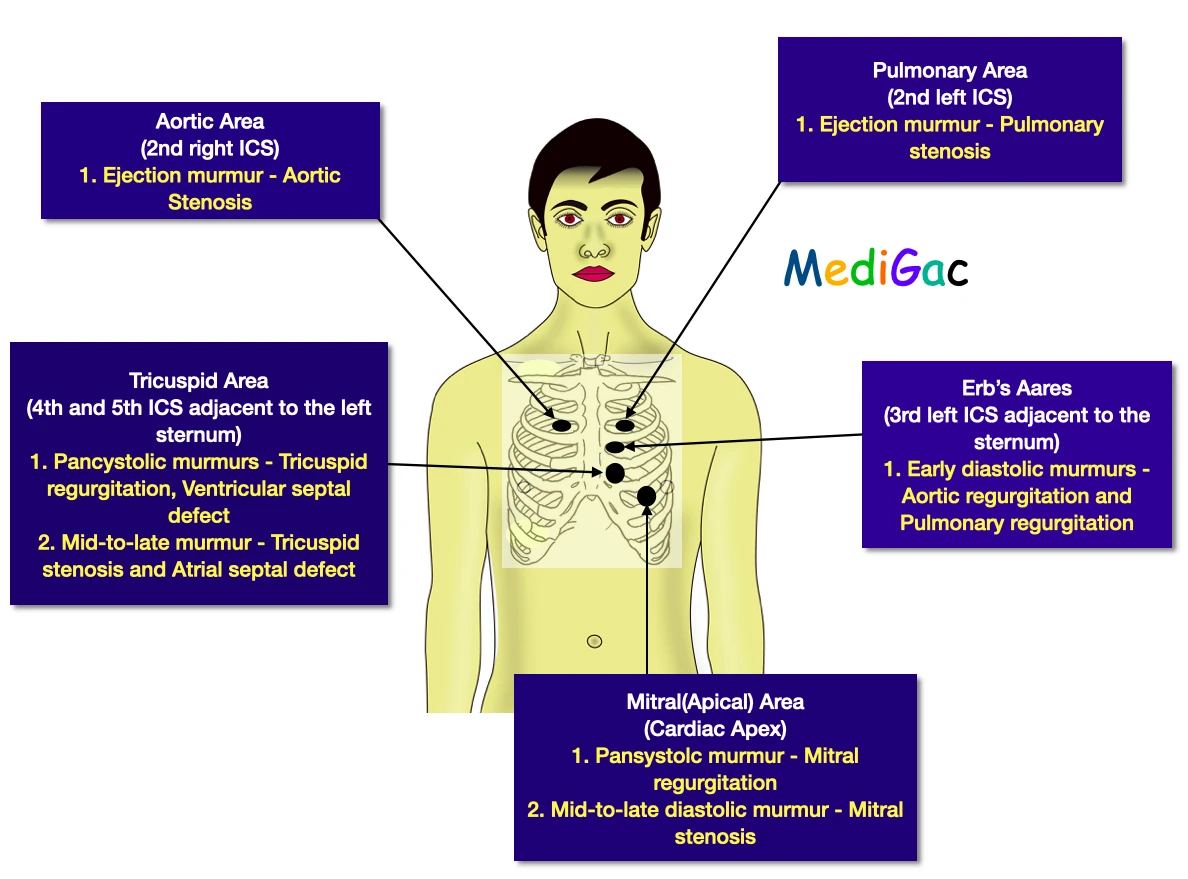
1. Aortic Area(2nd right Intercostal space) :
In aortic area of the chest we mainly heard ejection murmur.
- Ejection murmur – Aortic Stenosis
2. Pulmonary Area(2nd left Intercostal space) :
In pulmonary area, also we able to heard ejection murmur.
- Ejection murmur – Pulmonary stenosis
3. Tricuspid Area(4th and 5th ICS adjacent to the left sternum) :
- Pansystolic/Holosystolic murmurs – Tricuspid regurgitation, Mitral regurgitation and Ventricular septal defect
- Mid-to-late murmur – Tricuspid stenosis and Atrial septal defect
4. Erb’s Area(3rd left ICS adjacent to the sternum) :
- Easy diastolic murmur – Aortic regurgitation and pulmonary regurgitation
5. Mitral(Apical) Area(Cardiac apex) :
- Pansystolic murmur – Mitral regurgitation
- Mid-to-late diastolic murmur – Mitral stenosis
II. Mechanisms of cardiac murmurs :

You have already read the turbulence theory of fluid in your physics classes. The physics and mechanism of Murmurs totally based on sound theory and turbulence theory. As you can see that high water flow through narrow pipe causes production of sound, and also if any obstruction is given in the water flow stream then this will also cause formation of various sounds. Now we are mentioning all the three mechanism in briefly below.
- High blood flow through blood vessels.
- Forward flow with any narrowing of blood vessels or if any obstruction is present.
- back flow of blood through and incompetent valve or septal defect.
III. Grades of cardiac murmurs :
There are mainly six grades of Murmurs. They are described below :
- Grade 1 : These are known as faintest murmur or very soft murmurs which can be heard under optimal conditions. In character this murmurs are very soft, heard with difficulty and murmurs that only specialist cardiologists can heard.
- Grade 2 : These are soft and readily audible.
- Grade 3 : These are prominent murmur.
- Grade 4 : Loud murmur which also can be palpated.
- Grade 5 : These are loud and also can be heard with the stethoscope on the chest wall.
- Grade 6 : This the loudest murmur which can be easily heard by stethoscope also after removing the contact with the chest wall.
IV. Types of cardiac murmurs :
Mainly the murmurs are classifies into broad types, they are Systolic and Diastolic murmurs. And in others section we have discussed some special types of murmurs.
A. Systolic Murmurs :
- Midsystolic murmurs (Stenosis murmurs) : Aortic and Pulmonary Stenosis
- Pansyctolic/Holosystolic (Regurgitation murmurs) : Mitral and Tricuspid regurgitation
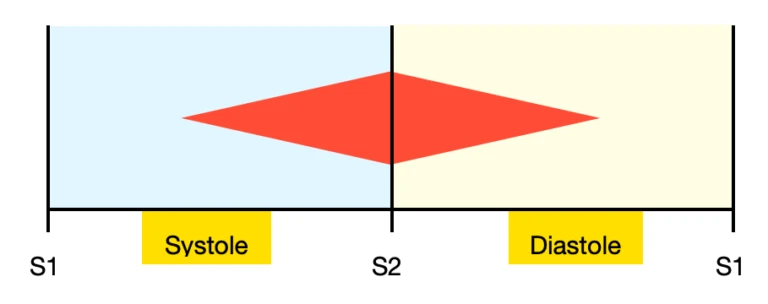
I. Midsystolic murmur(Systolic ejection murmur) :
S1 and S2 will be clearly audible because a midsystolic murmur occurs soon after the S1 heart sound and ends just before the P2 heart sound. Because many lesions that cause midsystolic murmurs are unrelated to systolic ejection, the term midsystolic is favoured over SEM.

Characteristics :
- Grade remains less than 3/6.
- Mid systolic peaking
- Mostly associated with anaemia
Occurs in :
- Aortic Stenosis
- Pulmonary stenosis
- Hypertrophic cardiomyopathy
- Aortic sclerosis
II. Pansystolic murmur :
From the S1 to the S2 heart sound, there is a murmur that lasts the entire systolic interval.

B. Diastolic Murmurs :
- Early diastolic (Regurgitation murmur) : Aortic and Pulmonary Regurgitation
- Continuous murmurs : Arteriovenous communication, Patent ductus arteriosus
- Mid-late diastolic (Stenosis Murmurs) : Mitral or Tricuspid stenosis
I. Early diastolic murmur :
These murmurs begins with the closure of the semilunar (aortic and pulmonary) valves at the same time as S2 and normally terminate before S1.

II. Continuous murmur :
During both systole and diastole, continuous murmurs can be detected. They happen when there is a persistent shunt between two blood vessels with different pressures.
III. Mid-late murmur :
Murmurs that begin after S2 and end before S1 are known as mid-diastolic murmurs. They occur as a result of turbulent flow through the atrioventricular (mitral and tricuspid) valves during the rapid filling phase caused by mitral or tricuspid stenosis.

C. Other Murmurs :
We have discussed this murmurs in the last of this post. So you will get each one in detail in the last part of this post.
V. Loudness of cardiac murmurs :
Loudness or intensity of murmurs can be simply increased and decreased. Now we will discuss when it will increase and decrease.
A. Increased loudness/intensity :
- High cardiac output like in hyperdyanamic state.
- Thin chest wall.
- Narrow diameter of thoracic cavity.
- Anemia (Blood velocity gets decreased)
- Tortuous aorta
B. Decreased loudness/intensity :
- Decreased cardiac output (congestive cardiac failure, low ejection reaction)
- Obesity
- Muscular or thick chest wall
- Obstructive lung disease
- Barrel shaped chest (Anteroposterior diameter gets increased)
- Pericardial thickening or fluid
Other cardiac murmurs :
I. Innocent Murmur :
As the name implies this murmur is related with children. It is mostly found in early age group and then slowly disappears when the children starts to grow.
No pathology of valve behind the formation of murmur. Mostly this occurs due to pulmonary vascular bed in children and increased heart rate which ultimately causes high-velocity blood flow.
Characteristics of Innocent murmur :
- Best heard over the Pulmonary area and localised
- Systolic in nature
- Normally grade II murmur that is soft and bowing.
- Best heard in supine position whereas it shows disappearance in upright position.
- And sometimes the murmur is heard after exercise, crying.
- No thrill is present
II. Functional Murmur :
This occurs due to increase flow of blood. It mainly shows the characteristics of localised murmur, Systolic murmur, Not very loud in intensity, Without any thrill, This murmur is reversible that is after correction of the blood flow the murmur shows absence, postural independent.
- Severe Aortic incompetence – Functional systolic murmur in Aortic area
- Aortic Stenosis disease – In the pulmonary, during systolic murmur
- Pulmonary hypertension – Early diastolic Graham Steell murmur
- Austin Flint murmur or Apical mid-diastolic murmur in a case of Aortic Incompetence
III. Haemic Murmur :
When a person has severe anaemia, an ejection systolic murmur can be heard in the pulmonary and aortic areas, this is known as Haemic murmur.
IV. Flow Murmur :
This is a physiological murmur, it means that is is not due to any pathological abnormality. Increased blood flow is frequently the cause of a flow murmur.
Flow murmurs are most common in babies, children, and teenagers. The murmur may persist into and throughout adulthood in rare situations.
This murmur best heard over the Pulmonary area and the major causes behind this occurrence are – Severe anaemia, Thyrotoxicosis, and Pyrexia.
V. Changing Murmur :
Sometimes characteristics of murmur does not remain constant and tends to show various changes, and these are called changing murmur.
Examples :
- Atrial myxomas
- Infective endocarditis
- Atrial ball valve thrombus