
Thyroid nodules are lumps or bumps in the thyroid gland. The majority of thyroid nodules are benign, but about two or three out of every twenty are malignant. Thyroid nodules can produce too much thyroid hormone, resulting in hyperthyroidism. Thyroid nodules that produce too much thyroid hormone almost always turn out to be harmless.
I. Clinical features of thyroid neoplasms
There are various clinical features of thyroid diseases. But incase of Benign or Malignant growth we mainly lie upon two things and that is – Swollen thyroid gland and Cervical lymphadenopathy.
II. Classification of thyroid neoplasms

As you know neoplasms can be Benign and Malignant both.
- Benign – Follicular adenoma
- Malignant – Primary and secondary. In Primary malignant neoplasm, there are Follicular papillary carcinoma, Medullary carcinoma, Lymphoma, and Anaplastic growth. In secondary, there are Metastatic carcinoma and Local invasion carcinoma.
1. Papillary carcinoma :
The most prevalent type of well-differentiated thyroid cancer is papillary carcinoma (PTC), which is also the most common type of thyroid cancer caused by radiation exposure. In a healthy thyroid parenchyma, papillary cancer shows as an irregular solid or cystic mass or nodule.
2. Follicular carcinoma :
After papillary carcinoma, follicular thyroid carcinoma (FTC) is the second most common thyroid malignancy. Differentiated thyroid cancers include follicular and papillary thyroid tumours, which account for 95 percent of thyroid cancer cases.
3. Medullary carcinoma :
Thyroid cancer that originates in cells that emit the hormone calcitonin is known as medullary carcinoma of the thyroid. “C” cells are the name for these cells. Inside the front of your lower neck is the thyroid gland.
4. Malignant lymphoma :
Thyroid primary malignant lymphoma is usually non-Hodgkin type and is frequently related with Hashimoto’s thyroiditis. Thyroid lymphoma is more frequent in women, with an average age of onset of 60 years. The most noticeable sign is a rapidly expanding goitre.
5. Anaplastic or undifferentiated carcinoma :
This is one of the most dangerous cancers in people. Thankfully, it appears to be uncommon. It can arise spontaneously or as a result of papillary or poorly differentiated carcinoma dedifferentiation. Rapid growth, visceral invasion, and distant metastases are all characteristics of the disease.
III. Diagnosis of thyroid neoplasm
- Enlarged lymph nodes – Cervical lymph nodes gets enlarged.
- Biochemical tests – Thyroid hormone level is assessed.
- USG – The nodules and structure of thyroid gland is examined carefully.
- FNAC – Fine needle aspiration cytology : This is a study of cells which is taken from thyroid mass or tissues.
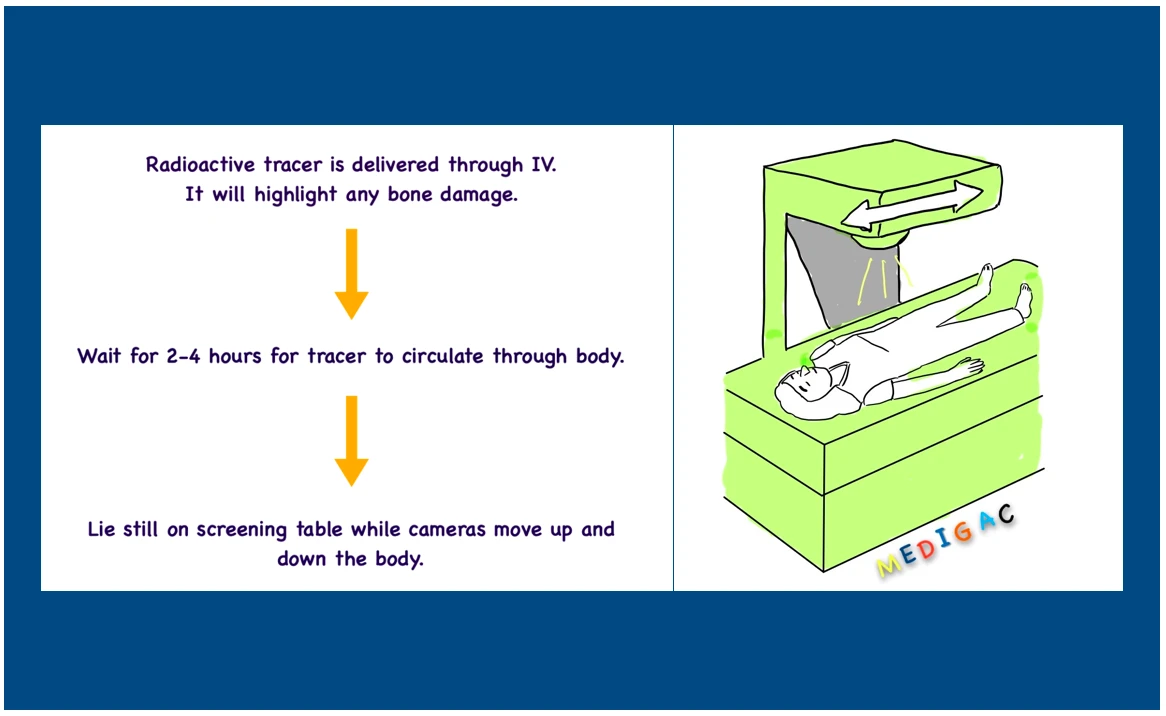
- Radio-Iodine Uptake scan – Radio active tracer is delivered through Iv route.
IV. Treatment thyroid neoplasms
Different treatments are available for different thyroid neoplasms.
I. Benign neoplasm :
This is treated with surgical removal of thyroid gland or total lobectomy. Tissues which remains appears to be normal so further following up seems to be unnecessary.
II. Malignant neoplasm :
1. Papillary carcinoma and Follicular carcinoma :
- For high risk patients – Total thyroidectomy will be performed in high-risk patients with nodal or distant metastases to eliminate illness in the thyroid and prepare the patient for radioactive iodine treatment.
- For low-risk patients – A thyroid lobectomy is an option for low-risk patients who have a single focus of disease that is restricted to the thyroid.
When metastatic illness is present in the neck, a therapeutic compartment-oriented neck dissection should be performed to remove disease from the central or lateral neck, depending on which side of the neck is involved.
Other than surgical treatment, Thyroxine and Radioiodine therapy can also be applied.
- Thyroxine treatment – Thyroid cells, both normal and cancerous, can be inhibited with high doses of thyroxine after surgery.
- Radioiodine therapy – Iodine is concentrated in thyroid tissue. As a result, X can be used to deliver tumoricidal dosages of radioactivity directly to benign and malignant thyroid tissue.
- Thyroglobulin – Discussed below.
Thyroglobulin :
- Normal thyroid cells and most differentiated thyroid tumours generate thyroglobulin, a tumour marker.
- As a result, this provides an exceedingly precise technique of monitoring patients after surgery.
- The level will not be undetectable if a lobectomy was performed, but patterns can be utilised to monitor for recurrence.
- The goal after a complete thyroidectomy is to have undetectable thyroglobulin.
- Patients who reach this point have a very low chance of recurrence.
- Patients can be monitored throughout follow-up using serial thyroglobulin measurements (6–12 monthly) along with ultrasound neck examination.
2. Medullary carcinoma :
Treatment for edullary thyroid cancer is determined by the cancer’s stage (how big it is and where it is in the body), the patient’s overall health, and the patient’s preferences. The treatment options for medullary thyroid carcinoma are discussed in this section. Three significant factors are used to make treatment decisions:
- What is the best treatment option for this type of medullary thyroid cancer?
- What are the wishes of the patient?
- What are the thyroid cancer team’s capabilities and outcomes?
- Total Thyroidectomy with central compartment lymph nodes (the lymph nodes beneath and surrounding the thyroid gland, breathing tube (trachea), and swallowing tube) for Medullary Thyroid Cancer Surgery (esophagus).
- Thyroidectomy (Extended or Complicated).
- For Cancer Spread to Lymph Nodes Along The Side Of The Neck, Medullary Thyroid Cancer Surgery (anterolateral neck).
- External Beam Radiation therapy for thyroid Cancer.
- Chemotherapy and/or targeted therapy.
3. Malignant lymphoma :
- Staging of the neck and chest should be done when medullary carcinoma is detected.
- When a patient’s condition is limited to the thyroid, a complete thyroidectomy to remove all C cells is advised. In addition, to improve the chances of cure, elective dissection of the central neck nodes is performed.
4. Anaplastic carcinoma :
- Isthmusectomy is the most appropriate form of biopsy in individuals with tracheal compression, yet the response to therapy is so rapid that this should rarely be necessary unless a histological diagnosis has been difficult to make.
- The prognosis is favourable, especially if no cervical lymph nodes are involved.