Fistula or sinus – Physical examination including the General and Systemic examinations step by step discussion along with all the possible differential diagnosis.
I.What are the possible diagnosis of a Sinus/Fistula :
A. Differential diagnosis of a Sinus:

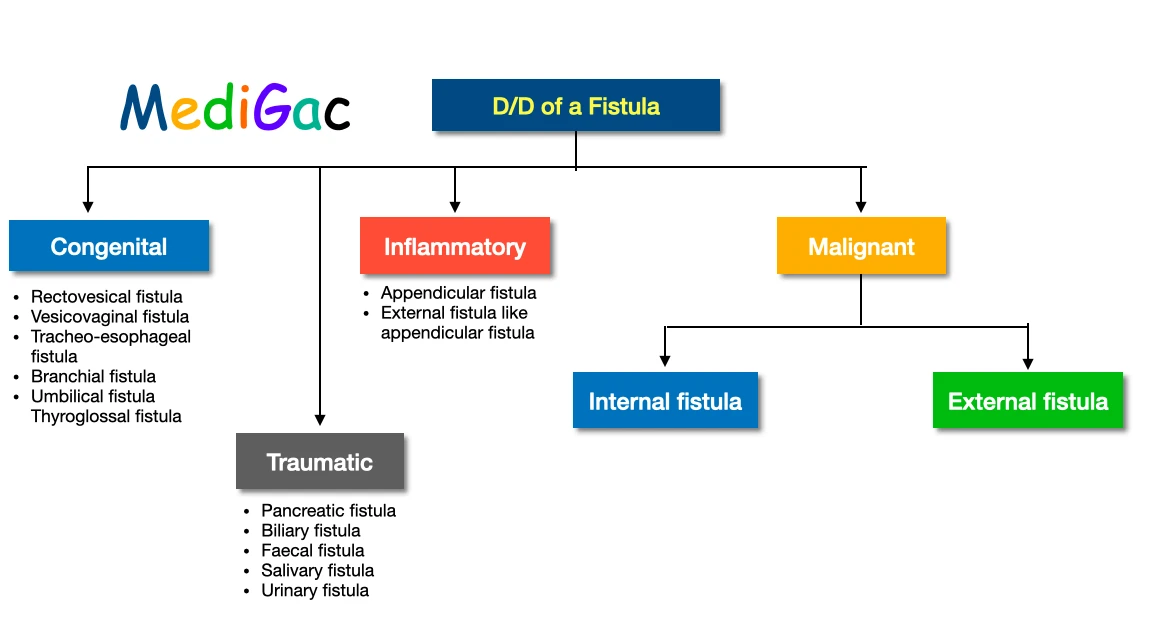
B. Differential diagnosis of a Fistula :
II. What are the General examination of a Sinus/Fistula :
Sinus examination :
- In the case of a sinus infection, the loin, spine, ribs, and kidneys should all be evaluated to determine the exact origin of the infection.
- The chest should be extensively inspected if a sinus is present due to chronic empyema.
- If the patient has a sinus infection caused by osteomyelitis, the examiner should have your bone inspected as stated under ‘Examination of bone illnesses.’
Groin Sinus examination :
In the event of groyne sinus, the hip joint and spine should be evaluated because it could be the result of a clod abscess bursting there.
Fistula examination :
In the event of a fistula around the anus, a thorough examination should be undertaken, including manual and proctoscopic examinations of the anal canal and rectum, as well as sigmoidoscopy and an inspection of the entire abdomen.
Multiple Fistula examination :
The lower urinary track should be thoroughly inspected if there are many fistulae in the perineum and scrotum.
III. What are the Systemic examination of a Sinus/Fistula :
We have discussed Inspection, Palpation, Probe examination and lymph node examination.
I. How to do the Inspection part :
1. Examination of the Number of fistula/Sinus –
Even though the vast majority of fistulae in the body are single, a few are infamous for their multiplicity.
These are the following:
- Water can perineum
- Ulcerative colitis is a condition that occurs in some people.
- Actinomycosis is characterised by the presence of numerous sinuses.
- Chron’s disease, which affects the rectum and anal canal and results in many anal fistulas.
2. Examination of the discharge from the fistula/sinus –
- It is always a good idea to check the discharge’s kind.
- It is frequently pustular in osteomyelitis.
- It is frequently serosanguineous in tuberculous ulcers, and the presence of sulphur granules in the discharge of actinomycotic sinuses is common.
- Urine, faeces, bile, and other bodily fluids may be visible pouring out of a fistula.
3. Examination fo the position of fistula/sinus –
Various sinuses can be diagnosed depending on the site of the fistula.
- Preauricular sinus – This is caused by a failure of fusion of the ear tubercles located at the root of the helix or on the tragus of the pinna, with the sinuses pointing upwards and backwards.
- Multiple indurated sinuses – This is located in the upper neck and indicates actinomycosis.
- Single sinus – Osteomyelitis is the most common cause of a single sinus above the lower uneven jaw.
- Tuberculous sinus – This sinus frequently assumes an unusual posture, indicating the diagnosis.
- Branchial fistula – This occurs when the second branchial arch fails to fuse with the fifth arch, which is almost always found in the lower portion of the neck, immediately in front of the sternomastoid muscle.
- Pilonidal sinus – Located behind the anus, this sinus is usually visible in the middle.
4. Examination of the surrounding skin of fistula/sinus –
- Scarring in the surrounding tissue could indicate chronic osteomyelitis or a previously healed tuberculous sinus, among other things.
- There may be dermatitis and pigmentation in the surrounding area, which are common in Crohn’s disease and actinomycosis.
5. Examination of the opening of the fistula/sinus –
- Sprouting granular tissue at the sinus aperture indicates the presence of a foreign body at the depth, such as sequestrum. For example, sequestrum, a drainage tube, a bullet, and so on.
- The aperture of a tuberculous sinus is often wide, with a thin blue and weakened edge.
II. How to do the Palpation part :
1. Examination of the mobility of the sinus/fistula –
Over the deep structures, the sinus mobility is checked. Osteomyelitis causes the sinuses to become attached to the bode, which becomes uneven, thickened, and painful.
2. Examination of the lump or swelling of the sinus/fistula –
Tuberculous lymphadenitis is commonly indicated by the presence of a lump in the vicinity of a sinus.
3. Examination of the tenderness of fistula/sinus –
If the sinuses are tender, this should be checked. Inflammatory sinuses are normally painful, similar to osteomyelitis.
4. Examination of the wall of the sinus –
This is palpated to see if there is any thickening. Because of the fibrosis that surrounds the sinus wall, chronic sinuses will have a thick wall.
III. How to do the examination with a probe :
This is crucial, but it should not be carried out without prudence. The clinician will learn the following from this examination :
- The presence of any foreign body in the depth of the wound, such as sequestrum, which is movable.
- Whether or not the fistula connects to a hollow viscus
- Whether or not a new discharge appears when the probe is withdrawn.
- The sinus’s orientation and depth.
IV. How to do the examination of draining lymph nodes :
The lymph nodes in the area should be thoroughly inspected.
IV. What are the Investigations to be done of a Sinus/Fistula :
- The discharge should be examined with proper investigation techniques
- X-ray examination can be done which may show Sequestrum and osteomyelitis changes in a bone.
- Sterilized methylene blue, Charcoal powder, and Coloured drug like pyridium may be used to make a confirmation on fistula.